Sample Letter Of Authorization To Access Medical Info
“`html
Letter of Authorization to Access Medical Information
This document serves as a sample letter of authorization. You should adapt it to your specific circumstances and consult with legal counsel if you have any concerns.
Introduction
A Letter of Authorization to Access Medical Information, often called a medical release form, is a legally binding document that grants permission to a designated individual or entity to review and obtain a patient’s protected health information (PHI). This is crucial for situations where the patient is unable to access or manage their medical records themselves, or when they need a trusted individual to advocate on their behalf. Such situations can arise due to illness, incapacity, travel, or simply a desire for assistance in navigating complex medical information. The Health Insurance Portability and Accountability Act (HIPAA) provides strict guidelines for protecting patient privacy, and this letter ensures compliance with those regulations by clearly outlining the scope and limitations of the authorized access.
Key Elements of a Medical Release Form
A well-drafted Letter of Authorization to Access Medical Information should include the following essential components:
- Patient Information: This section clearly identifies the patient whose medical records are being authorized for release. It includes the patient’s full legal name, date of birth, address, and other relevant identifying information. Accuracy in this section is paramount to avoid confusion and ensure the correct medical records are accessed.
- Authorized Representative Information: This section details the identity of the individual or entity who is being granted access to the patient’s medical information. It includes their full legal name, address, phone number, and relationship to the patient (e.g., spouse, parent, child, friend, attorney). Specifying the relationship is important for context and can influence the level of access granted.
- Scope of Authorization: This is arguably the most important section of the letter. It defines the specific types of medical information that the authorized representative is permitted to access. The authorization can be broad, covering all medical records, or it can be limited to specific conditions, treatments, or time periods. Examples include:
- “All medical records relating to [specific condition], including diagnoses, treatments, lab results, and progress notes.”
- “Medical records from [specific hospital or clinic] covering the period from [start date] to [end date].”
- “Information related to prescriptions filled at [specific pharmacy] between [start date] and [end date].”
- Purpose of Disclosure: This section explains why the patient is authorizing the release of their medical information. This provides context for the recipient and helps ensure that the information is used appropriately. Common reasons include:
- “For the purpose of assisting with medical decision-making.”
- “For the purpose of filing an insurance claim.”
- “For the purpose of seeking a second opinion.”
- “For the purpose of legal representation.”
- Expiration Date: The letter should specify an expiration date, after which the authorization is no longer valid. This prevents unauthorized access to medical information indefinitely. The expiration date can be a specific date, or it can be tied to a specific event (e.g., “until the completion of my insurance claim”). If no expiration date is specified, the authorization may be considered valid for a reasonable period, but it’s always best to include one.
- Right to Revoke: The letter must clearly state that the patient has the right to revoke the authorization at any time, in writing. It should also specify the procedure for revoking the authorization (e.g., by sending a written notice to the healthcare provider). This is a fundamental patient right under HIPAA.
- Signature and Date: The letter must be signed and dated by the patient (or their legal guardian, if applicable). The signature serves as proof that the patient has knowingly and voluntarily authorized the release of their medical information. The date is important for establishing the validity of the authorization.
Sample Letter of Authorization
[Your Full Name]
[Your Address]
[Your City, State, Zip Code]
[Your Phone Number]
[Your Email Address]
[Date]
[Healthcare Provider/Institution Name]
[Healthcare Provider/Institution Address]
[Healthcare Provider/Institution City, State, Zip Code]
RE: Authorization to Release Medical Information for [Patient’s Full Name]
To Whom It May Concern:
I, [Your Full Name], hereby authorize [Authorized Representative’s Full Name], residing at [Authorized Representative’s Address], with phone number [Authorized Representative’s Phone Number], and whose relationship to me is [Relationship to Patient], to access and receive my protected health information (PHI) as described below.
Patient Information:
Full Name: [Patient’s Full Name]
Date of Birth: [Patient’s Date of Birth]
Address: [Patient’s Address]
Scope of Authorization:
I authorize the release of the following medical information:
[Choose ONE of the following options and modify as needed:]
- Option 1 (Broad Authorization): All of my medical records held by [Healthcare Provider/Institution Name], including but not limited to, diagnoses, treatments, lab results, progress notes, and billing information.
- Option 2 (Limited Authorization): Medical records pertaining specifically to my treatment for [Specific Condition] from [Start Date] to [End Date], including [Specify Types of Records, e.g., diagnoses, treatment plans, medication lists].
- Option 3 (Specific Records): Only the following specific records: [Clearly list the specific record types and dates, e.g., “The MRI report dated January 1, 2024”, “All records related to my visit on February 15, 2024”].
Purpose of Disclosure:
The purpose of this disclosure is to [Clearly state the reason for releasing the information. Choose ONE and modify as needed]:
- [To assist with my medical decision-making process by providing [Authorized Representative’s Name] with the necessary information to understand my condition and treatment options.]
- [To allow [Authorized Representative’s Name] to file an insurance claim on my behalf.]
- [To allow [Authorized Representative’s Name] to obtain a second opinion from another healthcare provider.]
- [To provide my legal counsel, [Authorized Representative’s Name], with the necessary information to represent me in a legal matter.]
Expiration Date:
This authorization will expire on [Specific Date] or [Upon completion of [Specific Event, e.g., insurance claim processing]].
Right to Revoke:
I understand that I have the right to revoke this authorization at any time by providing written notice to [Healthcare Provider/Institution Name] at the address listed above. Revocation will not apply to information already disclosed in reliance on this authorization. The revocation should be sent via certified mail, return receipt requested, to ensure proof of delivery.
I understand that this authorization is voluntary and that I am not required to sign it. I also understand that [Healthcare Provider/Institution Name] may not condition my treatment on my signing this authorization, except in limited circumstances permitted by law.
Sincerely,
_____________________________
[Your Signature]
_____________________________
[Your Printed Name]
Witness (Optional):
_____________________________
[Witness Signature]
_____________________________
[Witness Printed Name]
Date: _____________________________
Important Considerations:
- State Laws: Be aware that state laws may have additional requirements or restrictions regarding medical information release. Consult with an attorney to ensure compliance with applicable state laws.
- HIPAA Compliance: This sample letter is designed to be consistent with HIPAA regulations, but it is your responsibility to ensure that it meets all applicable requirements.
- Legal Advice: This is a sample document and should not be considered legal advice. Consult with an attorney to obtain advice tailored to your specific situation.
- Record Keeping: Keep a copy of the signed authorization letter for your records.
- Delivery Method: Consider sending the authorization letter via certified mail, return receipt requested, to ensure proof of delivery.
“`
 724×1024 sample authorization letter medical records from authorizationletter.org
724×1024 sample authorization letter medical records from authorizationletter.org  1275×1650 medical authorization letter examples from www.examples.com
1275×1650 medical authorization letter examples from www.examples.com 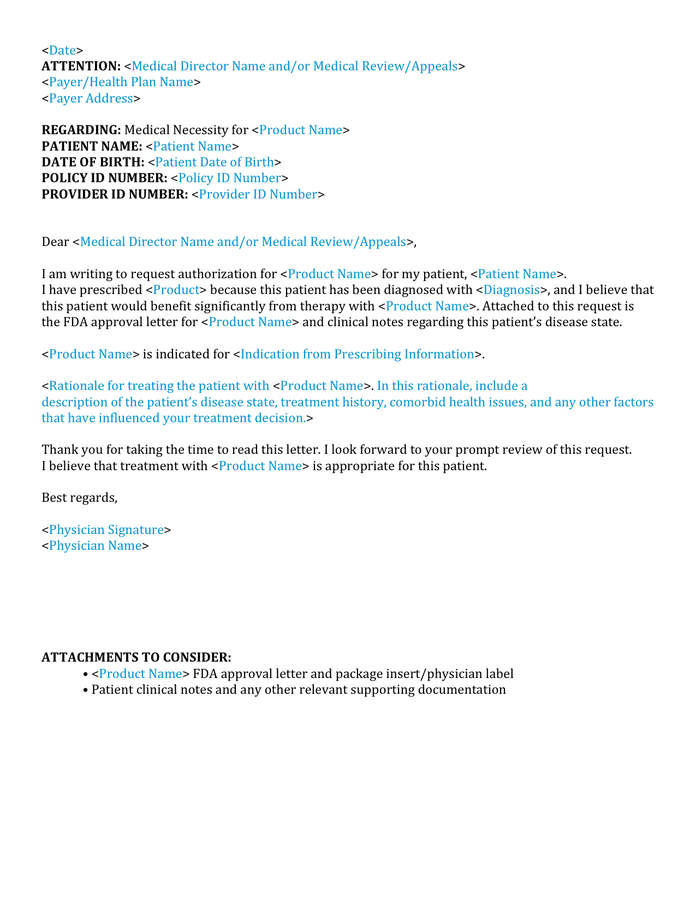 696×900 medical authorization letter sample word formats from www.dexform.com
696×900 medical authorization letter sample word formats from www.dexform.com  600×729 medical authorization letter examples format write from www.examples.com
600×729 medical authorization letter examples format write from www.examples.com  1275×1650 great authorization letter templates medical travel from templatearchive.com
1275×1650 great authorization letter templates medical travel from templatearchive.com  600×730 medical authorization forms word from www.sampletemplates.com
600×730 medical authorization forms word from www.sampletemplates.com  600×730 sample medical authorization letter templates from www.sampletemplates.com
600×730 sample medical authorization letter templates from www.sampletemplates.com  474×613 medical authorization letter template word excel from www.wordpdftemplates.com
474×613 medical authorization letter template word excel from www.wordpdftemplates.com  585×685 sample medical authorization letter templates ms word from www.sampletemplates.com
585×685 sample medical authorization letter templates ms word from www.sampletemplates.com  585×585 medical authorization letter printable zip from medicalletter22.blogspot.com
585×585 medical authorization letter printable zip from medicalletter22.blogspot.com  600×730 sample authorization letter template authorization letter from authorizationletter.net
600×730 sample authorization letter template authorization letter from authorizationletter.net  403×524 medical authorization letter templates word excel from www.wordpdftemplates.com
403×524 medical authorization letter templates word excel from www.wordpdftemplates.com 




Sample Letter Of Authorization To Access Medical Info :
Sample Letter Of Authorization To Access Medical Info was posted in November 26, 2025 at 2:51 pm. If you wanna have it as yours, please click the Pictures and you will go to click right mouse then Save Image As and Click Save and download the Sample Letter Of Authorization To Access Medical Info Picture.. Don’t forget to share this picture with others via Facebook, Twitter, Pinterest or other social medias! we do hope you'll get inspired by SampleTemplates123... Thanks again! If you have any DMCA issues on this post, please contact us!