Sample Letter Of Authorization For Medical Records
Sample Letter of Authorization for Medical Records
This document provides a sample letter of authorization for releasing medical records. It is essential to tailor this template to your specific needs and consult with legal counsel if you have any concerns regarding your privacy or legal rights.
Understanding Medical Record Authorization
A letter of authorization, often called a release form, is a legally binding document that allows a healthcare provider to share your protected health information (PHI) with a designated individual or entity. This is crucial because under HIPAA (the Health Insurance Portability and Accountability Act), healthcare providers are prohibited from disclosing your medical information without your explicit written consent, except in specific circumstances.
The authorization form outlines what information can be released, to whom it can be released, the purpose of the release, and the duration of the authorization. It’s a vital safeguard to ensure your medical privacy and control over your personal health information.
Why You Might Need a Letter of Authorization
Several situations might necessitate a letter of authorization for medical records, including:
- Sharing information with a new doctor: When you switch healthcare providers, your new doctor needs access to your medical history for informed treatment.
- Legal proceedings: If you are involved in a lawsuit, your attorney might need your medical records as evidence.
- Insurance claims: Insurance companies often require medical records to process claims.
- Family members needing access: In cases where a patient is incapacitated, a designated family member (e.g., with power of attorney) might need access to their medical records for care decisions.
- Research purposes: You may choose to donate your medical records for research, but only with your informed consent.
Key Components of a Medical Records Authorization Letter
A well-written authorization letter should include the following:
- Patient Information: Full legal name, date of birth, address, phone number, and other identifying information.
- Healthcare Provider Information: Name, address, and contact information of the healthcare provider or institution holding the records.
- Recipient Information: Name, address, and contact information of the individual or entity authorized to receive the records.
- Specific Records to be Released: Clearly specify the type of medical records to be released. Be as precise as possible. Examples include:
- Entire medical record
- Specific dates of treatment
- Consultation notes from a particular specialist
- Lab results (specify the type of lab tests)
- Imaging reports (e.g., X-rays, MRIs, CT scans)
- Medication list
- Immunization records
- Purpose of Disclosure: State the reason why the records are being released (e.g., for continued medical care, legal proceedings, insurance claim).
- Expiration Date or Event: Specify the date when the authorization expires. This could be a specific date, a certain period (e.g., one year from the date of signing), or upon the occurrence of a specific event (e.g., the conclusion of a legal case). If no expiration date is provided, the authorization may remain valid indefinitely, depending on state laws and the provider’s policies.
- Method of Disclosure: Indicate how you want the records to be transmitted (e.g., mail, email, fax, secure online portal). Be aware of potential security risks associated with unencrypted email.
- Right to Revoke: Clearly state that you have the right to revoke the authorization at any time by providing written notice to the healthcare provider. Explain the procedure for revocation.
- Statement of Understanding: A statement acknowledging that you understand that once the records are released, they may no longer be protected by HIPAA and could be subject to redisclosure by the recipient.
- Signature and Date: Your signature (or the signature of your legal representative, if applicable) and the date. If signing on behalf of someone else, you must clearly indicate your relationship to the patient and provide documentation of your legal authority (e.g., power of attorney).
Sample Letter of Authorization
[Your Full Name] [Your Address] [Your Phone Number] [Your Email Address] [Date] [Healthcare Provider's Name] [Healthcare Provider's Address] RE: Authorization to Release Medical Records for [Patient's Full Name], DOB: [Patient's Date of Birth] Dear [Healthcare Provider's Name or Medical Records Department], I, [Your Full Name], am writing to authorize you to release my medical records (or the medical records of [Patient's Full Name], for whom I am the legal guardian/power of attorney – *attach documentation of legal authority if applicable*) to the following recipient: [Recipient's Full Name] [Recipient's Address] [Recipient's Phone Number] [Recipient's Email Address] I authorize you to release the following specific medical records: [Choose one of the following options or modify as needed:] * My entire medical record held by your practice. * The following specific records: [List specific dates of service, consultation notes from Dr. [Doctor's Name], lab results from [Date] to [Date], imaging reports (e.g., X-ray, MRI, CT scan) taken on [Date(s)], medication list, immunization records, etc.]. *Be as specific as possible.* The purpose of this disclosure is for: [State the reason – e.g., continued medical care with a new physician, legal proceedings, insurance claim, personal records]. This authorization will expire on [Specific Date] OR [One year from the date of signing] OR [Upon the conclusion of [Specific Event, e.g., the legal case of [Case Name and Number]]]. I request that the records be transmitted via: [Choose one: Mail, Email (please be aware of potential security risks), Fax, Secure Online Portal]. If choosing mail: please send to the recipient's address listed above. If choosing email: please send to the recipient's email address listed above. If choosing fax: please send to [Fax Number]. If choosing Secure Online Portal, please provide instructions on how the recipient can access the records. I understand that I have the right to revoke this authorization at any time by providing written notice to your office. Revocation will not affect any actions taken prior to your receipt of the revocation notice. To revoke this authorization, I must send a written and signed revocation notice to [Healthcare Provider's Name] at [Healthcare Provider's Address]. I understand that once my medical records are released to the recipient listed above, they may no longer be protected by HIPAA and could be subject to redisclosure. Sincerely, [Your Signature] [Your Printed Name] *If signing as legal guardian or power of attorney, add:* Relationship to Patient: [e.g., Legal Guardian, Power of Attorney]
Important Considerations
- Review Carefully: Before signing any authorization form, carefully review all the information to ensure its accuracy and completeness.
- Keep a Copy: Make a copy of the signed authorization form for your records.
- Revocation: If you change your mind, you can revoke the authorization in writing. Send the revocation notice via certified mail with return receipt requested to ensure proof of delivery.
- State Laws: Be aware that state laws regarding medical record access and authorization may vary. Consult with an attorney if you have any questions about your rights.
- Seek Legal Advice: If you are unsure about any aspect of the authorization process, consult with an attorney or legal professional specializing in healthcare law.
This sample letter is for informational purposes only and does not constitute legal advice. Always consult with a qualified professional for guidance tailored to your specific situation.
 724×1024 sample authorization letter medical records from authorizationletter.org
724×1024 sample authorization letter medical records from authorizationletter.org  612×792 sample authorization letter template from authorizationletter.org
612×792 sample authorization letter template from authorizationletter.org  580×345 authorization letter template release medical records from www.free-power-point-templates.com
580×345 authorization letter template release medical records from www.free-power-point-templates.com  794×1058 medical authorization letter templates allbusinesstemplatescom from www.allbusinesstemplates.com
794×1058 medical authorization letter templates allbusinesstemplatescom from www.allbusinesstemplates.com  231×300 letter authorization release medical records sample templates from www.sampleletter1.com
231×300 letter authorization release medical records sample templates from www.sampleletter1.com  585×685 sample medical authorization letter templates ms word from www.sampletemplates.com
585×685 sample medical authorization letter templates ms word from www.sampletemplates.com 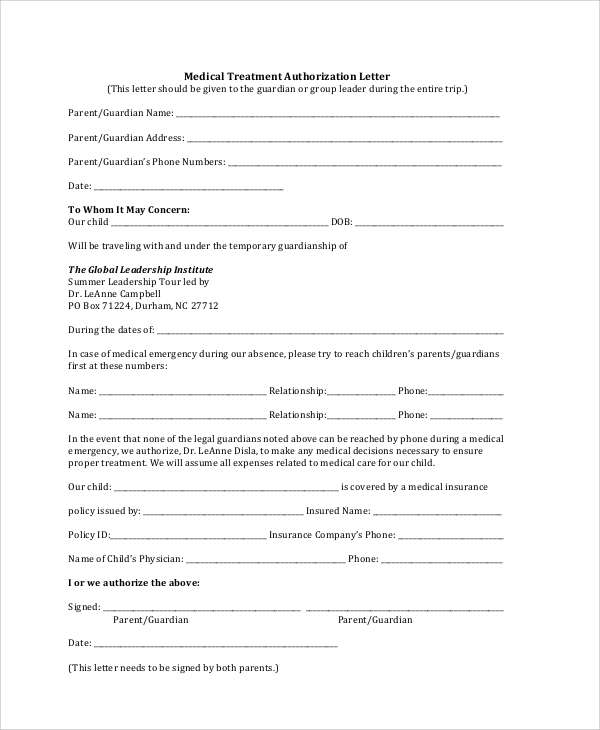 600×730 sample authorization letter template authorization letter from authorizationletter.net
600×730 sample authorization letter template authorization letter from authorizationletter.net 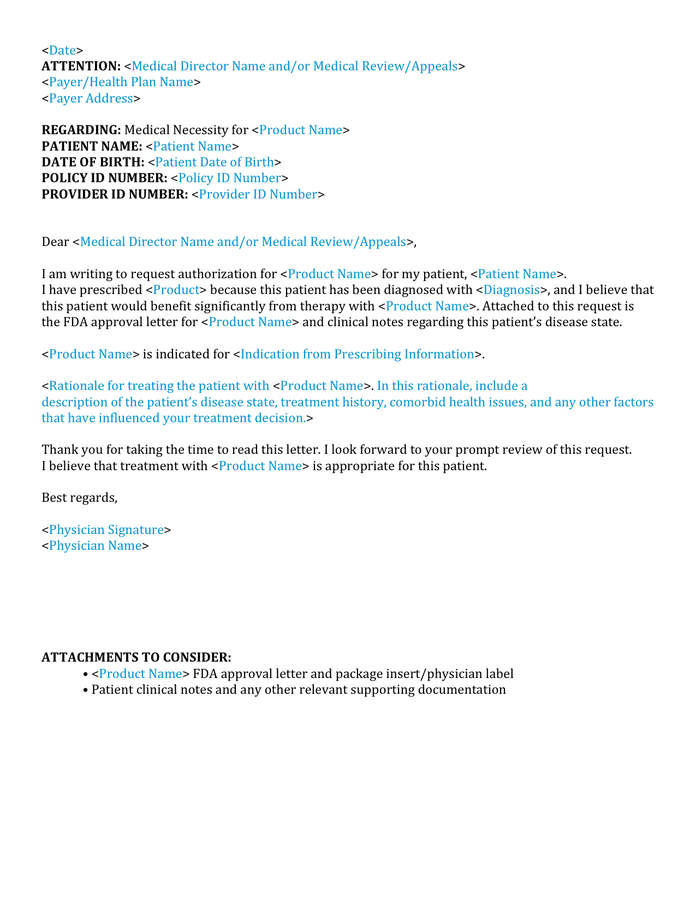 696×900 medical authorization letter sample word formats from www.dexform.com
696×900 medical authorization letter sample word formats from www.dexform.com  600×730 sample medical authorization letter templates from www.sampletemplates.com
600×730 sample medical authorization letter templates from www.sampletemplates.com  794×1123 printable authorization release medical records cover letter from www.printablelegaldoc.com
794×1123 printable authorization release medical records cover letter from www.printablelegaldoc.com  474×693 authorization letter release medical records sample from www.lettersformats.com
474×693 authorization letter release medical records sample from www.lettersformats.com 




Sample Letter Of Authorization For Medical Records :
Sample Letter Of Authorization For Medical Records was posted in September 9, 2025 at 10:58 pm. If you wanna have it as yours, please click the Pictures and you will go to click right mouse then Save Image As and Click Save and download the Sample Letter Of Authorization For Medical Records Picture.. Don’t forget to share this picture with others via Facebook, Twitter, Pinterest or other social medias! we do hope you'll get inspired by SampleTemplates123... Thanks again! If you have any DMCA issues on this post, please contact us!